
Dec 16, 2015
Dec 15, 2015
Great Question!
I get a lot of questions about stroke recovery and try to answer the best I can given the fact that I have rarely met the folks I'm giving advice to. Here is an email I got recently. Hope the following exchange helps some folks!
Dear Mr. Levine,
In March of 2014 my friend had a stroke. She is 59, very gifted and motivated. She has received physical and occupational therapy from local facilities since then and has made a lot of improvement. We have obtained a Neuromove unit and recently got a Walkaide device for her foot, but it is looking like we are reaching the limit of local expertise to help her push forward. She has been very motivated up to now, but upon not satisfactorily acheiving some of her 6 month goals, has hit a rough patch. So we are just searching for anything that might spur her on at this point. We have looked into constraint induced programs locally, but not impressed with what we have found. Also, she is very reluctant to undergo the frustration she thinks this therapy will be. We don't want to encourage her to do something difficult without knowing it has a good chance of helping her. I am writing to you because your book has been a huge help in "coaching" her, and I thought you might know someone in New England who we could go to for help.
"Joan"
Hi "Joan,"
A couple quick things; it looks like you're doing the right thing re: NeuroMove, and the walkaid. I'm a pretty big fan of both of those.
Secondly, if she is plateauing, that's to be expected. The general philosophy is that once the plateau has taken place, gains can continue to be made, but of course, the gains are much more conservative given an equal amount of work.
Sometimes it helps to work towards specific goals. For instance, your friend may walk great with the walkaid, but may not walk fast enough to make getting around outside useful. So increasing the speed of walking would be the goal. In fact, quickness can generally be used as a goal; upper body dressing, cooking a specific dish, making a bed etc. can all be goals were speed is worked on.
In terms of finding a place in New England, of course there are quite a few good ones. Find the link on this blog on the right hand column [-->] you'll see something that says "FIND A STROKE CENTER NEAR YOU?" Click on that, put in your ZIP Code, and all the hospitals that are supposed to be good at stroke recovery will come up- they should be able to direct you to the best rehab options. There's other links on there (on the right side column [-->]) to help you look for aggressive physiatry and other rehab clinicians.
One last thing, and this is a tough one… But your friend may be simply at the end of recovery. This is one thing I struggled with in my book… And in fact had somebody else write it; Kathy Spencer. I'll attach and image of her quote to this email (bottom of this blog entry). And she talks about the point at which living your life gets in the way of recovery. At some point there's not enough justification for the hard work given the amount of gains that are made. It's a decision that everybody has to make for themselves.
Have you looked into the saeboflex? It may be appropriate.
But, again,there's no magic algorithm here, it's just more work.
Please let me know if you have any other comments, insights, etc.
Best,
Pete
Pete
(CLICK ON TEXT BELOW TO MAKE IT LARGER!)

The Brain Science Podcast: The brain brought to you by the people who actually study it.
First, a bit of a acknowledgement:
Ginger Campbell wrote a very nice review of my book which
ended up on the book's cover. I asked her to write it because I love her podcast; The Brain Science Podcast.
The podcast, which is usually in interview form, is an incredible resource for anyone interested in the brain. Ginger Campbell, the creator/director, interviews lions of neuroscience at the top of their game. I rarely find myself lost in her question and answer tête-à-tête. She strikes the perfect middle ground where you understand what they're talking about but it's not simplified into mush.
Ginger Campbell wrote a very nice review of my book which
 |
| Ginger Campbell, MD |
The podcast, which is usually in interview form, is an incredible resource for anyone interested in the brain. Ginger Campbell, the creator/director, interviews lions of neuroscience at the top of their game. I rarely find myself lost in her question and answer tête-à-tête. She strikes the perfect middle ground where you understand what they're talking about but it's not simplified into mush.
In the negotiation to get her to write a blurb for my book, she floated the idea of me being interviewed on the Brain Science Podcast, to which I spat my coffee all over the computer screen. Sure, interview a whole bunch of people who are teetering on the verge of a Nobel, and then interview me. I've decided I'm a "science communicator." And in this regard me and Dr. Campbell have a lot in common. She's not a neuroscientist, she's not a neurologist, as I understand it she's an ER MD (see her update to this, below). So it's been sheer curiosity that has driven her to the brain. And we have that in common. Every other organ in the body is known-- right down to its molecular structure, we know what's going on. But the brain is not only unknown, it's really unknown.
Stroke has been the fascination of scientists since Hippocrates. Dr. Campbell has done several episodes on stroke but almost all the episodes has something relatable to stroke.
Please note, there is a link to the podcast on the right hand column (→)
Here is Dr. Campbell's input on this entry...
 "After spending over 20 years as an emergency physician I am now doing a Fellowship in Hospice and Palliative Care Medicine at the University of Alabama School of Medicine.
"After spending over 20 years as an emergency physician I am now doing a Fellowship in Hospice and Palliative Care Medicine at the University of Alabama School of Medicine.
Stroke has been the fascination of scientists since Hippocrates. Dr. Campbell has done several episodes on stroke but almost all the episodes has something relatable to stroke.
Please note, there is a link to the podcast on the right hand column (→)
Here is Dr. Campbell's input on this entry...
"After spending over 20 years as an emergency physician I am now doing a Fellowship in Hospice and Palliative Care Medicine at the University of Alabama School of Medicine.
However, I do need to clarify the difference between Free and Premium episodes, which I hope you will pass on to your readers.
The 25 most recent episodes are ALWAYS free. This represents about 2 years of content. Free episodes are available in iTunes, Stitcher, and most other podcasting apps.
There is some limited Premium Content in iTunes, but this is from 2010 when I was experimenting with making Premium versions of new episodes. (I also had CD's of these but they didn't sell so I quit after 3 episodes (65-67).
The Premium subscription ($5/month) gives people unlimited to all the back episodes PLUS episode transcripts. Details at http://brainsciencepodcast.com/premium. I also offer all these episodes and transcripts for $1 each. These have been more popular than expected.
Access to the Premium content is via a special webpage and/or via the mobile APP, which is now free.
I have gotten a few complaints about putting some of my content behind a Pay wall, but many more listeners appreciate having an easy way to support my work. I don't make that much but since I took a 50% paycut to pursue my Fellowship in Palliative Medicine, every little bit helps!
One other thing: even the premium episodes contain Audible ads because there is no easy way to remove this."
"Science. Confusing everyone since the 1500s!"
 |
| Girl. For no particular reason. |

Let's talk about stroke first. Current use of OC increases chance of a clot breaking of somewhere in the veins/arteries and causing stroke. Interesting side-note: Chances go up with the amount of estrogen in the OC. Nerdy way of saying this: "... the risk is directly proportional to the amount of estrogen present in the pill."
The article also says there is an increase in brain and breast cancers. Brain cancer chance IS doubled but the type of brain cancer they're talking about is very rare so a doubling still makes it ... very rare.
Breast cancer is increased but only if you are a recent user (within the prior year).
And what of the affect of oral contraceptives (OC) on stroke? "Current OC use increases risks of venous thromboembolism and ischemic stroke. However, women of reproductive age are at low baseline risk, so the chances are small."
And what of the affect of oral contraceptives (OC) on stroke? "Current OC use increases risks of venous thromboembolism and ischemic stroke. However, women of reproductive age are at low baseline risk, so the chances are small."
Hemianopsia (visual field cut) after stroke: The Neuroplastic model
Note: There are two free resources for retraining vision after stroke. Both are on the right hand column of this site (-->). Click on "Vision Problems? Click Here!" and/or "Tx for hemianopia and spatial neglect".
Sometimes survivors "neglect" their bad side. Survivors who have neglect don't pay attention (don't see or even recognize as their own) the "bad" side. In fact, it can be so bad that they don't even look at the "bad side" half of the world.

There are a ton of terms for this phenomenon. Unilateral neglect is the most common. Other terms are...
- unilateral spatial agnosia
- unilateral visual neglect
- hemi-inattention
- hemi-imperception
This inattention may be caused by visual deficits on the neglected side— a problem of the eyes and eyesight. The problem with eyesight that cuts off half the world is called hemianopsia.
Or it may be a matter that the brain is not processing information coming from that side, including vision. Or it could be both of those (vision and a brain problem) together.
Unilateral neglect and the brain
What do we pay attention to? There's lots of stuff in this great big world so we make choices about what we attend to. But someone with unilateral neglect can't/won't pay attention to their "bad" side.

The "neuroplastic model of stroke recovery" was a term I coined based on the observation that, no matter what deficits are left the survivor there are groups of researchers trying to develop "brain rewiring" treatments to reverse those deficits.
The neuroplastic model for Unilateral neglect becomes really clear if you look at it as more of a "won't" issue and less of a "can't" issue. If a survivor won't, it suggest that they could. Because if they won't then maybe their perspective can be changed so they will. So reducing inattention can be helped by paying more attention.
With unilateral neglect inattention to the affected side is bad for obvious reasons. But Inattention is also bad, because, as this book points out: Inattention results in confusion, and confusion increases inattention. So what can be done? How do you get someone or yourself, to attend; to pay attention?
Therapists contend that you should approach and do everything on the affected side so that the stroke survivor attends this affected side. However, it's a good idea to start off on the good side, otherwise, you may not know if the survivor is even paying attention to what you're trying to communicate with them. For instance the survivor may not understand instructions, context, spacial issues, etc. So do all the early teaching stuff on the good side.
To start with, survivors can be encouraged to turn their head towards the neglected side. Eventually, the survivor should be encouraged not to turn their head, but to move their eyes towards the neglected side.
It happens more often with people where the left side of their body is the "bad side." This may have something to do with the fact that we tend to be "right eye dominant." That is just in the normal course of human events, the right eye is the one that we more trust, and use.
Using tactile stimulation can help survivors be aware of the neglected side. You can use touch on the affected side, or rough cloth, a vibrator, etc.
It's a good idea for survivors to understand that they have neglected side. If it's a vision problem, be aware that you have vision loss on that side. Examples in the room around them can be used. You might say how many chairs in this room, and the survivor would only count half of them as they would neglect half the room, and therefore have the chairs.
Don't deny...
Nerdy take:
Bobath NDT: The bashing continues!

I know, I know, I bash NDT and Bobath a lot. I bash bloodletting too because it doesn't, whatchamacallit...work. That's it, work. It has the problem of not working. It is ineffective. It is devoid of efficacy. It is incapable of helping.
For a long time me and some colleagues in research got a ton o' backlash when we pointed out that the bird was dead. But more recently, PTs and OTs have generally got the message that its so dead, its starting to stank.
You know things are bad when Wikipedia turns on you! When you read this, have a look at two things: 1: The opening paragraph.

Its almost like the million Wile E. Cayote cartoons where he runs off the cliff and tries midair to run back to the cliff. 2: the rest of the page. Scath. Ing.
There are two ways to recover from stroke
There are two ways to recover from stroke. And they correspond to two of the four phases of stroke.
Let me start with four phases of stroke:
1. Hyperacute
2. Acute
3. Subacute
4. Chronic
For the sake of brevity let's cross off the top two:
Let me start with four phases of stroke:
1. Hyperacute
2. Acute
3. Subacute
4. Chronic
For the sake of brevity let's cross off the top two:
Recovery doesn't really happen during those two.
(I'll put why those two phases are important - outside of recovery per se- at the bottom of this entry).
Recovery – broadly defined as "getting better" – happens during the subacute and chronic phases.
Recovery – broadly defined as "getting better" – happens during the subacute and chronic phases.
The subacute phase: (from approximately the first week to approximately the third month –although this can vary wildly from survivor to survivor)
Most recovery during this phase is what would be called "spontaneous recovery" or "natural recovery." Recovery during this phase is driven by healing in the brain. Specifically it has to do with neurons that are temporarily "stunned" by the stroke becoming "unstunned" and coming back online. As they come back online recovery happens. That is, it's "spontaneous." It is true that people who get therapy during the subacute phase will get better than people who don't get therapy. In fact, people who get intensive therapy – therapy that involves a lot of work and a lot of repetitions – will get better than people who just get regular therapy. But even with no traditional therapy, survivors will almost always have some significant amount of recovery during the subacute phase. Lte's put it this way...
The subacute phase: Recovery Happens
The chronic phase (from approximately three months to the end of life).
Most recovery during this phase is what would be called "spontaneous recovery" or "natural recovery." Recovery during this phase is driven by healing in the brain. Specifically it has to do with neurons that are temporarily "stunned" by the stroke becoming "unstunned" and coming back online. As they come back online recovery happens. That is, it's "spontaneous." It is true that people who get therapy during the subacute phase will get better than people who don't get therapy. In fact, people who get intensive therapy – therapy that involves a lot of work and a lot of repetitions – will get better than people who just get regular therapy. But even with no traditional therapy, survivors will almost always have some significant amount of recovery during the subacute phase. Lte's put it this way...
The subacute phase: Recovery Happens
The chronic phase (from approximately three months to the end of life).
During the chronic phase a lot of recovery can happen. This phase was traditionally known as the phase in which nothing could happen – but that has been proven to be broadly untrue. What confuses people is that recovery doesn't happen as easily during the chronic phase as it did during the subacute phase. There is (usually) no "spontaneous" recovery during the chronic phase. The survivor has to claw and scratch for every bit of recovery. And while during the subacute phase spontaneous recovery is driven by neurons flooding back, during the chronic phase brain plasticity (rewiring) comes into play. And brain plasticity during chronic phase is just as difficult for the survivor as it is for the rest of us. It involves a lot of hard work, a lot of dedication, a lot of repetitions, and a lot of focus.

The hyperacute and acute phases.
Important things happen during these two phases, to be sure. Things like saving lives and saving brain. But these two phases are not conducive to the effort needed to drive recovery. In fact, if too much effort is made, you can enlarge the area damaged by the stroke. So during these two phases, listen to the healthcare professionals around you, and convalesce. But once the subacute phase starts, its time to "put the pedal to the metal."
How will you know when the subacute phase starts? Spontaneous recovery happens!


Don't worry, therapists...
I was doing a series of talks- on stroke recovery, natch- in Georgia last week. Someone brought up a concern about my talk that I also heard last time I did a series of talks. Here's a paraphrasing of that concern:
"You're saying that a lot of what we do in the clinic is shown to be ineffective in research. Payers (insurance/Medicare/Medicaid) are going to hear about this and then... I'm afraid we're going to get paid less and have fewer treatment options."
And I laughed. On the inside because out loud would have been rude. But: How silly! To think that insurance companies are listening to researchers about what is and is not effective! Insurance cares about shareholders and Medi"care" cares about keeping costs as low as possible. One thing they care little about: the science.
Therapists, fret not. Things that research indicates are ineffective are still paid for. Consider splinting. These are the rigid pieces of plastic that keep a joint in a certain position. They are believed to reduce muscle shortening in patients that posture in a flexed potion.
So people like this:

Get one of these...

Governmental clinical guidelines suggest splints don't work, and may make things worse. Its usually stated like this....
For stroke survivors at risk of or who have developed contractures and are undergoing comprehensive rehabilitation, the routine use of splints or prolonged positioning of muscles in a lengthened position is NOT recommended.
Is splinting paid for. Let's put it this way.

So relax therapists. Don't worry, they're not listening to researchers!
And not only will they pay for stuff that does not seem to work, they won't pay for stuff that does work yay!
Take constraint induced therapy (CIT). We've known for a while that is particularly effective for some stroke survivors. In fact, CIT shows up on every set of clinical guidelines in the English speaking world. Here for example, are the clinical guidelines for OT in Australia. Open it, and search (Ctrl+F) for the word "constraint."
Is CIT paid for? No. There is not even a "code" for it (a code is the numbers used to bill for a particular treatment).
"stroke recovery expert"
Use your hand. Now.
Even if you can't open your “bad” hand, you should use it.
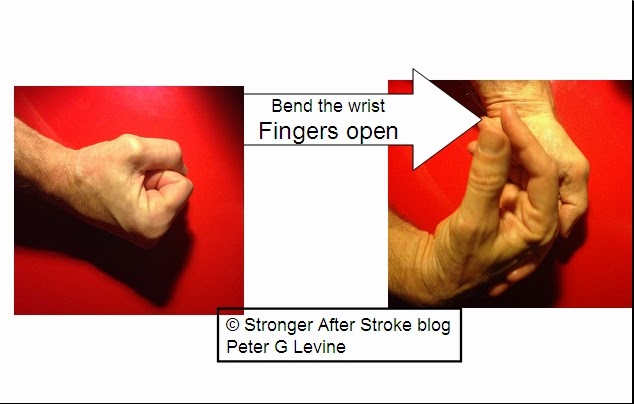 You can release your hand by using the “good” hand to bend the “bad” wrist. This maneuver typically opens the fingers. Once the fingers are open you can use the hand to stabilize, grasp, and even exercise. Grasping objects is, generally speaking, good for the hemiparetic hand. Squeezing objects, as well, is good for the hemiparetic hand.
You can release your hand by using the “good” hand to bend the “bad” wrist. This maneuver typically opens the fingers. Once the fingers are open you can use the hand to stabilize, grasp, and even exercise. Grasping objects is, generally speaking, good for the hemiparetic hand. Squeezing objects, as well, is good for the hemiparetic hand.


Using a gripping aid has two immediate benefits after stroke:
You can release your hand by using the “good” hand to bend the “bad” wrist. This maneuver typically opens the fingers. Once the fingers are open you can use the hand to stabilize, grasp, and even exercise. Grasping objects is, generally speaking, good for the hemiparetic hand. Squeezing objects, as well, is good for the hemiparetic hand.
One way you can quickly get the hand back in the game is using gripping aids. One company that makes a gripping aid that is very easy to use is Active Hands. (Full disclosure, Active Hands a sponsor of this blog).
Using a gripping aid has two immediate benefits after stroke:
- The “bad” hand can be used to augment your available grip to make gripping safer. The gripping aids would be just that; and aid. As much as you can, use the grasp you have to hold items. But the gripping aid can support your active grasp adding safety and functionality to the grasp.
- The hand, now “in the game” with the gripping aid, will now use the rest of the arm (shoulder, elbow, forearm rotation). In this way, the rest of the arm is used, which is good for recovery of the rest of the arm. The primary reason for the existence of the arm is to get the hand to where it needs to be, so a (a-HEM!) active hand leads to an active arm. And an active arm is one that is likely to recover.
Socializing, Play and Moving Helps Drive Recovery
Part of your recovery may depend on how much fun your having while you recover.

Enriched environments (EE) are what we all want. It's why we send our kids to good schools, why we seek out new experiences and why we travel. It turns out that enriched environments are very good for the brain. One of the main enrichments of environment that humans have is social interaction.
What do enriched environments have to do with stroke recovery? A ton.
What hurts social interaction? A stroke.
It turns out that there's pretty good evidence that stroke survivors engaged in enriched environments recover more. More than what,you may ask. Survivors involved in environments rich in social interaction, physical activity, and interesting experiences recover more than survivors who are not in enriched environment.
There is one caveat… Most of this research has been done on animals. The reason was done in animals is that it would be impossible to do the same sort of research and humans. Imagine a human study like this would go…
You would have to groups:
The control group: survivors would be involved in a highly social environment in which there were a lot of games played, a lot of conversations and a lot of physical activity.
The experimental group: survivors would be put in a cell where they were fed well, but did not engage any other humans in anyway.
A study like that on humans would be considered… What's the word? Unethical. That's the word: Unethical.
How do you find rats that have had a stroke? You give them one. Researchers surgically cause a stroke in the rats. (video here)
They then separated the rats into an experimental

and control group.

(Note: the idea of enriching environments is beginning to be tested in human survivors. It is made ethical by letting one group do what they normally would do while the experimental group got an increase in physical, cognitive, and social activity.)
What does the research show about the effect of enriched environments on stroke recovery? The rat stroke survivors in the enriched environments had better proprioception (sense of movement) than the rats that were left to themselves.
Also...
Recovery depends on neuroplasticity? Yeah...not entirely.

There's this idea among many clinicians and survivors that when it comes to recovery it's all about neuroplasticity. Certainly, my book as well as many of my articles support this concept. But it's not 100% true. Some of recovery comes from stuff other than neuroplasticity.



{kind=link}
I miss my old self (too)
One of the laments that I hear a lot from survivors is "I miss my old self." But please, survivors, keep in mind – we all miss our old self.
 |
| I feel grrrreat! |
 | ||
| I am as indestructible as I feel! |
We often tend to look at the past fondly simply because we were young. But we're all getting older, slower, achier – and- as if tipping our hand of our aging interior – our looks take a hit.
So let's say a stroke survivor had their stroke 10 years ago – when they were 40. Now they're 50, and they "Miss their old self." It is true that stroke ages you immediately. The estimate I read recently is that the stroke itself ages you at least five years. That is, your brain is five years older, your body is five years older, etc. – all within the first 24 hours of stroke. So when survivor say "I miss my old self," I can dig it.
 |
| Doing well! |
I haven't had a stroke, but I can tell you, 50 ain't 40. That is, you wouldn't be how you remembered irrespective of the stroke. So when you compare, compare to the projection of yourself given the added age.
So, like the rest of us, as you work against the deficits of the stroke you are also working against father time.
 |
| Crap I didn't even know I had aches. |
I do know some stroke survivors who are in some of the best shape of their life after their stroke because this was really the first time in their life that they look after themselves.